Understanding Infant Eczema and Current Research
Overview of atopic dermatitis (eczema)

Atopic dermatitis is more commonly known as atopic eczema or eczema.
Eczema is a chronic (life-long), inflammatory, itchy skin condition that presents in infants and early childhood. The condition typically fluctuates in severity between periods of flares and remissions. Eczema affects approximately 15-30% of children worldwide,¹ with variability in prevalence and severity by country.²
A family history of eczema is the most significant risk factor, increasing the risk by 2-3 times³. A family history means having at least one parent with eczema.
There are various gene changes that affect the skin barrier and immune response, increasing the likelihood of eczema. Environmental factors, such as allergens and other irritants, can trigger and exacerbate symptoms, leading to flare-ups.
Atopic dermatitis results from a complex interplay between environmental and genetic factors

What is Whole Goat MilkFormula (WGF)?
Whole goat milk formula or WGF refers to infant or follow-on formula in which whole goat milk is used as the only source of protein and ~50% of fat is from milk fat, rather than relying on isolated milk proteins (skim milk and whey) or vegetable oils.
Its defining features include the preservation of the natural 20:80 whey-casein protein ratio of goat milk and retention of a high proportion of milk fat (~50%).
This means that the whole goat milk formula (WGF):
✓ Has lower levels of key milk allergens, αS1-casein and β-lactoglobulin.
✓ Is more efficiently digested, lowering the allergic trigger potential.
✓ A post hoc analysis of the TIGGA study showed a trend for one-third lower cumulative incidence of eczema over 12 months in infants fed whole goat milk formula.
Introducing the Goat Infant Formula and Eczema (GIraFFE) Study
Main objective: To assess the effect of infant feeding with whole goat milk or cow milk infant formula on atopic dermatitis development during the first year of life.
Other objectives: Parameters for child growth, sleep, gastrointestinal symptoms, nutrition, quality of life, and blood and stool health markers are being measured until 5 years of age.

ClinicalTrials.gov registration number: NCT04599946
GIraFFE Study design
The GIraFFE Study™ is a multicenter, randomised, double-blind, controlled nutritional trial (Study Protocol).
Infants were recruited before the age of 3 months and randomly assigned to receive New Zealand made whole goat milk formula or cow milk formula. Only healthy full-term infants whose parents had chosen to initiate formula feeding for reasons unrelated to the trial. There were no selection criteria related to the risk of atopic dermatitis. Caregivers and their child completed assessments at either in-person visits or phone calls every two months, up to the age of 12 months, and periodically thereafter.
The study is being undertaken by trained study personnel and principal investigators at each study site. Growth measures and adverse events are conducted in accordance with Good Clinical Practice. Precautions were taken to ensure that the recruitment process did not interfere with breastfeeding intention or practices.
For the primary outcome measure for atopic dermatitis, the required sample size of 1,722 infants was calculated based on an atopic dermatitis incidence of 15% and a 30% risk reduction. A dropout of up to 25% was initially assumed, leading to a planned enrollment of 2,296 infants. However, recruitment was stopped after reaching a total of 2,132 infants, as the observed dropout rate was lower than initially assumed.
Intervention formula: Whole goat milk formula with 20:80 whey:casein ratio and ~50% milk fat as total fat
Control formula: Standard cow milk formula with 60:40 whey:casein ratio and vegetable oil as the predominant source of fat (milk fat 5% of total fat)
Overview of atopic dermatitis assessment of children to 12 months of age
Adapted from Ferry, et al. 20234
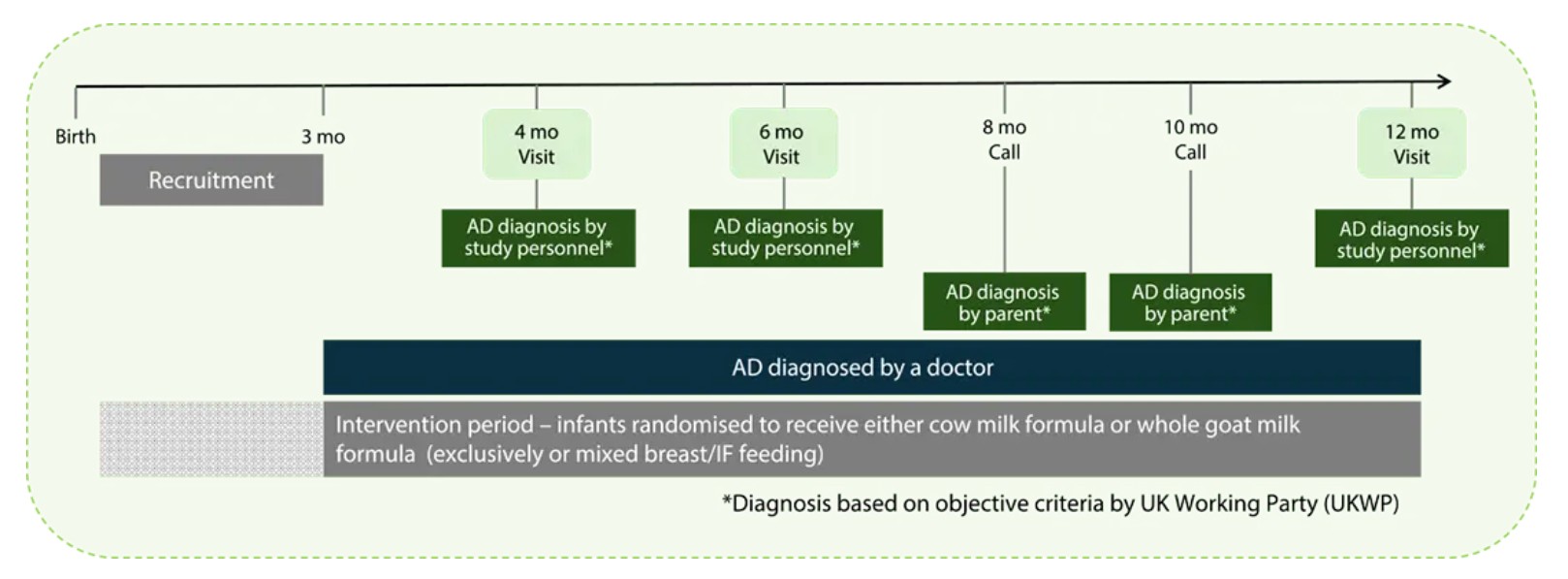
For the outcomes related to eczema, the participants were assessed for atopic dermatitis by several methods:
ADPRIMARY is the primary outcome and the strictest measure. Trained staff use the UKWP diagnostic criteria during face-to-face visits with infants at three time points (4, 6, and 12 months) to assess atopic dermatitis. To diagnose eczema under the UKWP criteria, a child must exhibit itchy skin and at least three of the following symptoms: dry skin, eczema in skin creases, a family history of asthma or hay fever, and visible eczema. Diagnosis based on objective criteria from the UK Working Party (UKWP), capturing only some forms of AD and/or AD present at study visits.
ADUKWP includes two additional time points, eight and ten months, where trained staff lead the parents through the UKWP examination of their toddler during a phone call.
ADDOCTOR was any AD that was diagnosed by a doctor up to 12 months of age. This captures any occurrence at any time, as evaluated by a trained practitioner, representing normal clinical practice. AD diagnosed by a doctor captures infants developing AD at any time throughout the intervention period.
ADANY combines all the data, representing the total number of infants identified as having AD by one of the measures. Note that an infant diagnosed by two or more methods they are only counted once.
Collaborative clinical study
The GIraFFE Study is led by the Comprehensive Childhood Research Center, Ludwig-Maximilians-Universität, Munich.
The Study involves 10 university groups across Poland and Spain, with experience in clinical trials and led by Principal Investigators with expertise in infant and childhood nutrition.
This work is supported by Dairy Goat Co-operative (NZ) Limited and the New Zealand Ministry for Primary Industries as part of the Caprine Innovations NZ Sustainable Food & Fibre Futures Partnership Programme (grant number PGP06-16001).
Learn more about eczema
Eczema is not simply a “rash” – it is a recurring, inflammatory condition with significant impact on children and their families.
The other impacts of eczema include:
- Infections of broken skin
- Reduced quality of sleep
- Affected psychological health & cognitive performance
- Missing school days and social events
- Increases the risk of other allergies
- Economic burden due to treatment
Eczema is not just a childhood disease. – Approximately 10% of infants and children with eczema will continue to experience eczema throughout their adulthood¹.
In addition, they are predisposed to other allergic diseases such as food allergies, asthma, and hay fever⁵. This is often referred to as the allergic march or multimorbidity.
- The risk of food allergies is 6 times higher in children with atopic dermatitis.
- The risk of asthma and hay fever is more than 1.5 times higher.
Prevention is the most effective way to reduce the burden of eczema and the development of other allergic conditions.
- Exclusive breastfeeding for at least 4-6 months has a protective effect of breastfeeding in the general population of infants and provides even greater protection for infants with a family history, with ~40% reduction⁶.
- Hydrolysed formulas may reduce the risk of eczema in infants with a family history by up to 25%⁷⁻⁸.
- Supporting the skin barrier with the use of emollients soon after birth (e.g. those that include ceramides), and the use of water softeners can provide benefits for infants at high-risk of eczema⁶.
The GIraFFE Study is investigating whether Whole Goat Milk Formula (WGF) can reduce the risk of developing atopic dermatitis/eczema compared to standard cow milk formula.
Reference
1 Bieber N Engl J Med 2008, 358, 1483-1494
2 Silverberg et al. Asthma & Immunology 2021, 126(4), 417-428
3 Ravn et al. J Allergy Clin Immunol 2020,1182-93
4 Ferry et al. BMJ open 2023, 13(4), e070533
5 Tsuge et al. Children 2021, 8(11), 1067
6 Chu et al. J Allerg Cin Immun 2024,12(7), 1695-1704
7 Li et al. Advances in Nutrition 2024, 15(5), 17
8 Vandenplas et al. Journal of pediatric gastroenterology and nutrition 2024, 78.2:386-413




